A) Discussion:
1- Is a high flow vascular malformation with abnormal arteriovenous shunting with no intervening capillary bed.
2-Communication could be either by a nidus or fistulous communication.
3-At imaging, the nidus appears as tortuous bag of warm appearance with early arterial and venous enhancement.
4-Complications include hemorrhage, infarction, seizures and hydrocephalus.
5- Spetzler- Martin Grading for post operative evaluation by evaluating nidus size as follow:
1 point: < 3 cm, 2 points: 3- 6 cm, 3 points: > 6 cm.
Venous drainage: (0 point: superficial, 1 point: deep).
Eloquence of adjacent brain (0 points: non eloquent, 1 point: eloquent).
Martin grades range from 1 to 5, with 6 being reserved for non operative candidates.
B) Diagnosis:
-AVM.
C) Imaging:
D) Dynamic study of AVM:
MR-DSA methodology was modified from Aoki et al (19). Sixty images were obtained using an RF-spoiled 2D Fourier-transformation steady-state technique, which permits one image per second. Imaging parameters for the gradient-echo sequence were 7/2 (TR/TE), a 40° flip angle, a 23-cm FOV, a 256 × 150 matrix, and a slice thickness of 6 to 10 cm. The phase sample ratio was 1.0 and the bandwidth was 50.0 kHz. Slices were orientated to give projections equivalent to those produced by CCA. In any given imaging domain (axial, lateral, reverse Towne), one run was conducted as a mask and a second run was obtained during the passage of a bolus of 6 to 10 mL (concentration, 0.5 M) of gadopentetate dimeglumine followed by a 10-mL saline flush. A separate contrast bolus was used for each anatomic projection. This was administered at a rate of 3 mL/s via a power injector (Medrad Spectris, Medrad, Netherlands) through an 18-gauge intravenous cannula inserted into the antecubital fossa vein (21). The quantity of contrast material varied according to nidus size, as determined from the standard fast spin-echo images, to optimize nidus visualization: 6 mL of full-strength gadopentetate dimeglumine was used for small (<3 cm) AVMs and 10 mL for medium-sized (3–6 cm) AVMs. After imaging, the mask run for a particular imaging plane was subtracted from the contrast run using proprietary software, and then viewed using video reversed cine. A maximum of 20 mL of gadopentetate dimeglumine was administered to any one patient.
Reference 1
Reference2
1- Is a high flow vascular malformation with abnormal arteriovenous shunting with no intervening capillary bed.
2-Communication could be either by a nidus or fistulous communication.
3-At imaging, the nidus appears as tortuous bag of warm appearance with early arterial and venous enhancement.
4-Complications include hemorrhage, infarction, seizures and hydrocephalus.
5- Spetzler- Martin Grading for post operative evaluation by evaluating nidus size as follow:
1 point: < 3 cm, 2 points: 3- 6 cm, 3 points: > 6 cm.
Venous drainage: (0 point: superficial, 1 point: deep).
Eloquence of adjacent brain (0 points: non eloquent, 1 point: eloquent).
Martin grades range from 1 to 5, with 6 being reserved for non operative candidates.
B) Diagnosis:
-AVM.
C) Imaging:
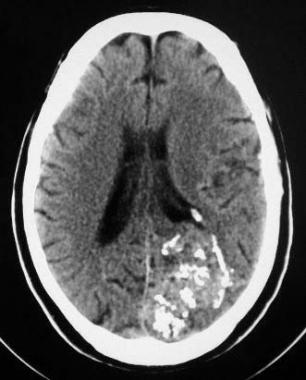 |
| A CT scan of the head that demonstrates a left occipital arteriovenous malformation (AVM), with multiple calcified phleboliths and numerous hyperattenuating vascular channels. |
 |
| Arteriovenous malformation (AVM) of the brain. An axial T2-weighted MRI showing numerous flow voids corresponding to the CT findings (not shown). Note the mass effect on the lateral ventricle despite the lack of a mass or hemorrhage. |
D) Dynamic study of AVM:
MR-DSA methodology was modified from Aoki et al (19). Sixty images were obtained using an RF-spoiled 2D Fourier-transformation steady-state technique, which permits one image per second. Imaging parameters for the gradient-echo sequence were 7/2 (TR/TE), a 40° flip angle, a 23-cm FOV, a 256 × 150 matrix, and a slice thickness of 6 to 10 cm. The phase sample ratio was 1.0 and the bandwidth was 50.0 kHz. Slices were orientated to give projections equivalent to those produced by CCA. In any given imaging domain (axial, lateral, reverse Towne), one run was conducted as a mask and a second run was obtained during the passage of a bolus of 6 to 10 mL (concentration, 0.5 M) of gadopentetate dimeglumine followed by a 10-mL saline flush. A separate contrast bolus was used for each anatomic projection. This was administered at a rate of 3 mL/s via a power injector (Medrad Spectris, Medrad, Netherlands) through an 18-gauge intravenous cannula inserted into the antecubital fossa vein (21). The quantity of contrast material varied according to nidus size, as determined from the standard fast spin-echo images, to optimize nidus visualization: 6 mL of full-strength gadopentetate dimeglumine was used for small (<3 cm) AVMs and 10 mL for medium-sized (3–6 cm) AVMs. After imaging, the mask run for a particular imaging plane was subtracted from the contrast run using proprietary software, and then viewed using video reversed cine. A maximum of 20 mL of gadopentetate dimeglumine was administered to any one patient.
 |
54-year-old patient with Wyburn-Mason syndrome and bilateral mirror-image parietal AVMs.
A, Axial T2-weighted (2900/87.5/2) image shows flow voids in both AVMs and the set-up acquisition block for the anteroposterior projection MR-DSA. Note that the anterior cerebral arteries are not included.
B, Right carotid selective conventional catheter angiogram shows the right-sided AVM.
C–E, Several stages of MR-DSA during the passage of a contrast bolus in a Towne projection. Early arterial phase (C), late arterial phase (D), and early venous phase (E).
|
Reference 1
Reference2